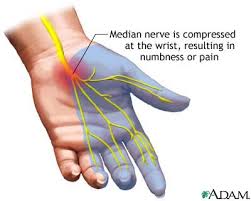
CARPAL TUNNEL SYNDROME – A condition that results from the compression of the median nerve as it passes through the carpal tunnel. Results in numbness in the median distribution — lateral 3 ½ digits.
The Carpal Tunnel:
- Just distal to wrist creases
- Floor is carpal bones, roof is flexor retinaculum ( aka transverse carpal ligament)
- Flexor retinaculum attaches to pisiform and hook of hamate medially, scaphoid and trapezium laterally.
- As the median nerve passes through the Carpal Tunnel, a branch runs above the flexor retinaculum. This branch is the Palmar Cutaneous branch. It supplies the skin over the thenar eminence
- Therefore, with CTS, the sensation over the thenar eminence is not affected.
Structures that Pass Through the Carpal Tunnel:
- Median nerve
- 4 tendons of flexor digitorum superficialis
- 4 tendons flexor digitorum profundus
- One tendon for flexor pollicis longus
– Compression occurs when the size of tunnel decreases, the size of the tunnel contents increases, or both.
MEDIAN NERVE:
- Receives contributions from C5 to T1
- The motor branches supply pronator teres and most of the muscles responsible for wrist and finger flexion
- The median nerve supplies motor innervations to the muscles of the thenar eminence and the first 2 lumbricals.
- The palmar digital and cutaneous branches supply sensation to the lateral 3 ½ digits and the distal palm respectively.
Causes of Carpal Tunnel Syndrome:
Carpal Tunnel Syndrome: Causes that lead to increase size of contents in tunnel:
- Repetitive flexion and extension of the wrist leading to edema, chronic fibrosis/ thickening of the tendons.
- Thickening of the retinaculum due to scar tissue from repeated trauma
- Systemic edematous conditions – diabetes, hypothyroidism, RA rheumatoid arthritis, pregnancy
Carpal Tunnel Syndrome: Causes that lead to decrease in tunnel space:
- Bony callous after carpal/ radial fracture
- Space occupying lesions- ganglia, lipoma, cyst
- Bony changes with Rheumatoid Arthritis
Carpal Tunnel Syndrome: Acute Causes
- Secondary to trauma ( fracture, dislocation of lunate)
- Infection
- Flareup of RA carpal tunnel massage
SIGNS AND SYMPTOMS of Carpal Tunnel Syndrome:
- Often unilateral — usually dominant hand
- Nocturnal dysthesia — abnormal sensation, often wakes person from sleep. ( can occur from sleeping with wrist flexed)
- Local pain, with wrist activity. Sometimes pain present in forearm and elbow secondarily
- Wrist ROM is decreased due to pain
- Person will shake/ massage the hand to relieve symptoms
- Swelling may be present
- Changes in tissue health in hand/ forearm
- HT/ TP in forearm flexors d/t overuse
- Adhesion in flexor retinaculum and tendons passing through tunnel
- As the condition progresses, atrophy of thenar muscles
- Sensory symptoms: numbness/ tingling in lateral 3 ½ digits ( may be burning pain/ heat). Thenar eminence is not involved. They can still feel it at the distal part or area distal to thenar eminence. (Thenar muscles still involved).
Carpal Tunnel Syndrome: OBSERVATIONS
- May wear a splint
- Edema local to hand/ wrist, may be over forearm
- Muscle atrophy and decrease tissue health in later stages
- Weakness in thenar mm. noted with client difficult holding pen/ writing
Carpal Tunnel Syndrome: PALPATION
- Signs of inflammation at wrist. In chronic, may be ischemic
- Tender local to the carpal tunnel
- Tissue may be boggy at wrist ( edema)
- Fascial restriction, HT, TP, in forearm mm
- Thenar atrophy in later stages carpal tunnel massage massage for carpal tunnel massage
Special TESTING: carpal tunnel massage
- AFROM, PRROM decreased in flexion, extension, possibly ulnar deviation
- AR strength testing of andictpr pollicis brevis decreased if CTS is chronic
- Phalen’s Test
- Reverse Phalens Test
- Cyriax Variation Test
- Geoff Aikin’s Test
- Tinel’s sign for median nerve
CONTRAINDICATIONS for Carpal Tunnel Massage:
- Frictions with anti-inflammatory medication is contraindicated
- Vigorous joint play if rheumatoid arthritis has resulted in joint hypermobility – is contraindicated
- Local massage for 10 days post corticosteroid injection is contraindicated
Carpal Tunnel Massage Therapy Treatment:
- Decrease hypertonicity in the forearm
- Fascial spreading massage techniques to flexor retinaculum to free up space
- A little bit of joint play to loosen up carpal bones
- Distal massage to prevent atrophy and for tissue health
- Hydrotherapy depends on stage of condition
- Cold — acute, inflamed, edema, post deep technique
- Contrast- vascular flushing
- Heat- before fascial work
- Acute Carpal Tunnel Syndrome – treat like any other acute condition: cold hydro, no on-site/ distal work. Treat proximal
- Insertions of flexor retinaculum treated with thumb kneading. If adhesion is located, treat with frictions. The retinaculum itself may be frictioned, do not compress median nerve. If numbness and tingling occur while you are frictioning an area, stop because you are on a nerve and compressing it.
- If muscle tone and tissue health is good, fascial work on the palm using spreading strokes. Followed by finger kneading, muscle stripping to palm and fingers.
- Joint play to elbow, carpals, metacarpal joints
- Chronic Carpal Tunnel Syndrome- most patients usually need chronic carpal tunnel massage.
- Begin with treatment to shoulder girdle, subscapularis, scalenes ( all have Trigger points that refer to the hand)
- Manual Lymphatic Drainage in the presence of edema
- MFR, Myofascial release – skin rolling to Forearm flexors and extensors – ( do not overwork and cause inflammation).
- Muscle stripping, ischemic compressions to muscles in the forearm, release any trigger points that refer to the hand. carpal tunnel massage
Muscle Trigger Point Referral:
- Trigger points that refer to thumb and lateral hand: scalene, brachialis, brachioradialis, opponens pollicis, adductor pollicis, palmaris longus
- Trigger points that refer to the wrist — subscapularis, flexor carpi radialis, pronator teres
SELF CARE for Carpal Tunnel Syndrome:
- Computer positioned so wrists in neutral and forearms parallel to the floor
- Ice applied during & after activity of forearms. Contrast hydrotherapy can flush out edema/ metabolic waste
- Frequent stretching of forearm flexors/ extensors
- Strengthening of forearm flexors and extensors once ROM of wrist has improved
- Self massage of forearms, retinaculum, palm
- Stress reduction. Acupuncture, chiropractor Carpal Tunnel Massage